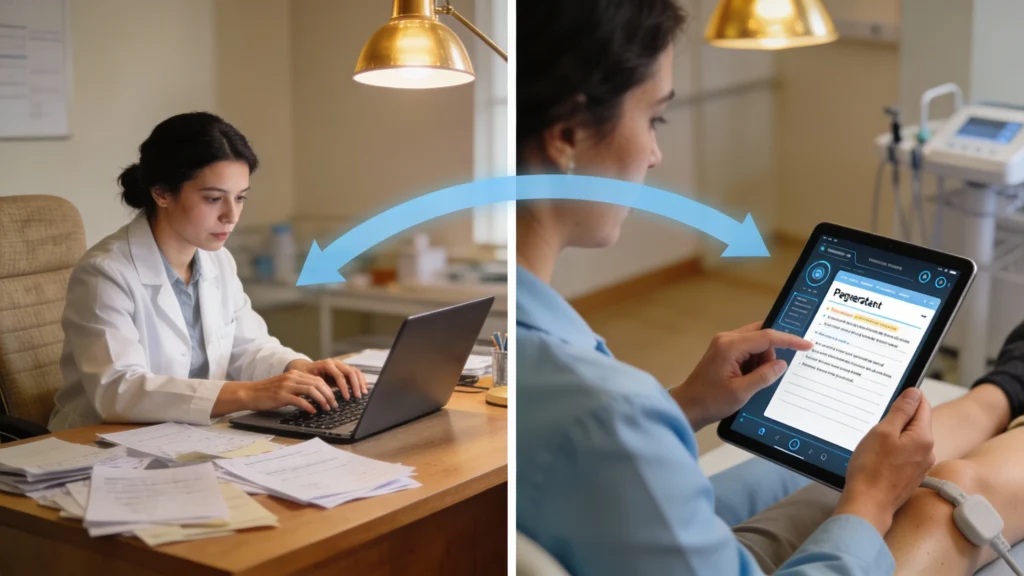
During evaluations, AI tools can listen to the therapist–patient conversation and automatically organize key details into history, objective findings, assessment, and plan. Instead of typing every word, the therapist reviews and edits a draft note, preserving clinical reasoning while offloading the repetitive parts of documentation to the software.
AI for physical therapy documentation refers to software that listens to patient encounters, analyzes therapist input, and generates structured notes aligned with clinical and billing standards. These platforms typically combine large language models, domain-specific templates, and coding logic tuned to outpatient orthopedics, neurorehabilitation, or acute care. The goal is to transform free-flow conversations and observations into defensible documentation without forcing therapists into rigid point-and-click screens.
Core Technologies Behind AI Documentation
Most systems start with medical-grade speech recognition, similar to Dragon Medical One or Amazon Transcribe Medical, which converts spoken words to text with 95–98% accuracy in quiet rooms. Natural language processing then identifies clinical concepts such as ROM measurements, manual therapy techniques, or gait deviations. These concepts are mapped into SOAP or ICF-based structures, while rule engines check for required elements like duration, assistive devices, and patient response.
Deployment Models in PT Settings
Clinics can access AI documentation through embedded EMR features, standalone web apps, or dictation add-ons. Embedded tools in systems like WebPT or Clinicient automatically store drafts in the patient chart, reducing copy-paste steps. Standalone tools may offer richer customization but require HL7 or FHIR interfaces, often costing $100–$250 per provider monthly. Dictation plug-ins integrate with existing templates, giving therapists incremental automation without a full system change.